On this week's broadcast of Mountain Stage, host Kathy Mattea looks back on some of her favorite archival sets from 2006 featuring The Derek Trucks Band, Bettye LaVette, Soulive (featuring Reggie Watts), Grace Potter & the Nocturnals, and more.
Home » Stories » In West Virginia’s Poorest Communities, The State’s Vaccine Rollout Has Left Vulnerable Residents Behind
Published
In West Virginia’s Poorest Communities, The State’s Vaccine Rollout Has Left Vulnerable Residents Behind
Share this Article
This story was originally published by Mountain State Spotlight. For more stories from Mountain State Spotlight, visit www.mountainstatespotlight.org.
Veronica and Carl Allen have lived in Wyoming County their entire lives. Like many residents of the state’s southern coalfields, they’re older and have health problems that make them especially vulnerable to COVID-19. For months they’ve lived in fear that they might contract the virus.
Last week, they got a glimmer of hope. On Jan. 13 Gov. Jim Justice made vaccinations available to people 70 and older.
But there was a problem. Instead of getting the vaccine through a local doctor or the county health department, Veronica and Carl were told they’d need to drive more than two hours from their home in Clear Fork to Greenbrier County.
“I was really sorry to hear that they sent our vaccines to Lewisburg,” Veronica Allen said. “I couldn’t stand a trip like that. There’s no way.”
The Allens aren’t alone. In an effort to accelerate the distribution of COVID-19 vaccines to West Virginians, the state has been holding a series of centralized vaccination clinics in January, mostly focused in the state’s most populous counties. This is the latest pivot in the state’s vaccination plan, following a surprise announcement at the end of December that left health departments scrambling to begin vaccinating the general public.
“We have been successful in vaccinating tens and tens of thousands,” said Justice, who has been making the rounds in national media coverage of the state’s vaccination successes. “We’re just going to stay right on that.”
But the approach has come with significant downsides. The state’s centralized facilities are less accessible to West Virginians living with high rates of poverty and pre-existing conditions which make the coronavirus especially lethal. Only one of the 10 poorest counties in the state has had a vaccine distribution clinic anytime in the last three weeks, according to an analysis by Mountain State Spotlight.
Map by Ian Hodgson
/
Poorest counties
Last week, Dr. Clay Marsh, the state’s coronavirus czar, acknowledged the problems.
“We need to continue to push vaccines to the communities where people live,” Marsh told Mountain State Spotlight. “It certainly sounds like we need to give more help to the folks in McDowell County and Lincoln County and other places.”
And on Thursday, the state announced plans to expand its vaccination hubs so there would be one in each of West Virginia’s 55 counties by early February.
Until then, Justice is urging everyone who’s eligible to make use of the existing vaccination clinics, but health care workers say the current hub system has placed certain West Virginians at an unfair advantage and left rural residents to fall behind.
“The thing that really makes my blood boil is that there’s not equal access,” said Dr. Joanna Bailey, a family physician who serves residents in Wyoming and McDowell — two of the state’s most impoverished counties.
Several of her patients lack access to transportation or have physical ailments that make traveling long distances difficult, if not impossible. But leaving the county is a requirement if patients want to be vaccinated soon.
Last week, Lewisburg was the designated vaccination site for residents living in nine counties, including Bailey’s patients in McDowell and Wyoming.
“There’s no chance in hell that my poor patient from McDowell County is going to be able to travel to Lewisburg on a day’s notice to get a vaccine,” Bailey said. “If the state wants to set up vaccine clinics rather than going through local providers or health departments, that’s fine, but make it fair and make it accessible.”
Despite dozens of vaccines being designated for patients from McDowell County, only three residents on a list of more than 100 were able to make the trip, a health department official said.
A similar problem arose in other counties, too. In Lincoln County where elderly residents who wanted to be vaccinated had to drive up to 45 minutes to Cabell County or go without the vaccine.
“This system is not only unacceptable, but morally wrong for the people that don’t live in one of the counties selected to be a hub,” said Allen Holder the director of emergency services operations for Lincoln County. “Lives in the country matter, too.”
With little notice, some health departments were left unequipped, understaffed and without a communication system in place to efficiently take calls, book appointments and answer questions. In some places, senior citizens waited in lines for hours. In others, some patients were mistakenly given antibody shots — used to treat coronavirus patients — rather than vaccines.
Despite these challenges, demand for the vaccine was plenty. And in more rural counties like McDowell, Wyoming and Lincoln, health officials were vaccinating residents quickly. The biggest question they had was when they’d be getting more doses.
Courtesy
/
McDowell County Health Department. Photo courtesy McDowell County Health Department
Those doses never came. The state pivoted and sent large quantities of vaccine to centralized locations in more populous areas instead of distributing smaller numbers of doses equally among all 55 counties. Marsh says it’s largely a matter of logistics.
“Our goals are to create a series of locations that would be able to conveniently serve the population of West Virginia,” he said. “As we are trying to immunize people in the state that aren’t at a facility like a big hospital or big nursing home, we are trying to create vaccine [hubs]… that everybody in West Virginia could access.”
Doing so effectively, said Marsh, requires a large quantity of vaccines, which the state has not received yet. Right now, the clinics are as good as it gets, Marsh said.
The state is planning to address these inequities in early February when it anticipates more doses will become available.
But in the interim, West Virginia’s older rural populations are still waiting.
“If we are only allotted 20 vaccines, that’s fine. Give us 20 vaccines and we’ll get them in people’s arms,” said Bailey, the doctor serving residents in the state’s southernmost counties. “But don’t say ‘there are 50 [for people from McDowell] but they have to travel to Greenbrier to get them.’ That makes no sense. It seems like vaccines are being administered to patients who have the most resources instead of the least.”
Bailey said it’s a sign of both systemic inequality and racism built into health care. Most of her older patients live with chronic diseases that make them more likely to die if they contract COVID-19.
Chronic illnesses like heart and lung disease are especially concentrated in the state’s poorer rural counties. Data analysis by Mountain State Spotlight found that McDowell County has the second-highest rate of resident deaths due to cardiovascular disease and respiratory disease in the state, topped only by Mingo County, which also went without vaccines.
Map by Ian Hodgson
/
Sickest counties
Wyoming County had the third highest rate of residents to die from chronic respiratory disease.
Of the 46 clinics to be announced by the state since Jan. 7, only two — in Logan County on Jan. 21 and 22 — will take place in any of West Virginia’s 10 poorest counties.
Poverty isn’t the only factor affecting health. National data shows that Black communities are far more likely to suffer from pre-existing conditions that make the coronavirus lethal. Black residents are also more likely to work in retail and service positions where they may be exposed to the virus.
Yet data on state vaccine distribution shows that Black residents in West Virginia have been vaccinated at about half the rate of white residents in the state.
In the absence of data
Although West Virginia is currently leading the nation in its vaccination rate, and gaining accolades for doing so, the state has primarily aimed for the low-hanging fruit, beginning with health care workers and nursing home staff, and now including some teachers and those who work in higher education.
But as the state receives more doses of the vaccine and moves to vaccinate the general population — people 65 and older as of Jan.19. — the task becomes trickier.
“When you have to get the vaccine distributed out as widely and as quickly as possible, the inequities that already exist have the potential to be further amplified,” said Dr. Elizabeth Miller, director of adolescent and young adult medicine at the University of Pittsburgh Medical Center.
Miller has been heading an initiative to encourage vaccination in under-resourced communities.
“Rural communities have been devastated by lack of access to preventive services and comprehensive care,” she said. “It is absolutely critical that rural communities are front and center of vaccine distribution.”
Miller said the key is to find balance between getting the vaccine out as quickly as possible through major distribution hubs — which is what West Virginia is currently doing — and prioritizing the most vulnerable residents who may be difficult to reach. That, she said, is best accomplished through communication with the people working on the ground.
“We have to rely on leaders in our rural communities and listen to them in terms of where and who should be leading the vaccine distribution planning in those areas,” Miller said.
Shweta Bansal, a disease ecologist at Georgetown University, said the choice to target more densely populated areas through vaccine hubs could more rapidly reduce the spread of the coronavirus, but not necessarily drastically decrease mortality.
“One of the arguments for vaccinating in urban centers first would be to prioritize those who transmit most,” Bansal said. “[But] it’s actually quite clear that we really should be prioritizing the most vulnerable first. And the rationale isn’t just an ethical one.”
Evidence from past infection outbreaks shows that prioritizing vulnerable populations like the elderly and those with pre-existing conditions is the best way to reduce the number of deaths.
Like Miller, Bansal said the best way to reach these populations is through direct outreach by health care providers who already serve the community.
One problem researchers like Miller and Bansal see is a lack of data to monitor who is getting vaccinated and where.
West Virginia’s COVID-19 dashboard, maintained by the state Department of Health and Human Resources, displays the number of vaccines distributed by age group and race, but does not record where vaccinations were administered or the number of residents vaccinated by county.
“Data transparency opens doors to more responsive and targeted vaccination campaigns,” said Bansal, who helped develop COVID-19 Vaccination Tracking which collects vaccination data from across the country. Data tracked by her team shows that at least eight states, including Ohio, Illinois and Florida are reporting vaccination data by county, and Bansal said that more should follow suit.
“Without detailed vaccination data, we will continue to be a few steps behind the devastation that the virus is causing,” Bansal said.
‘I just hope I can get that vaccine real soon’
Both experts in-state and out will tell you that rapid vaccine distribution is really hard. It will get better with time.
But the lag-time has its costs, and those costs are being borne by the most disadvantaged residents.
Everyday without the vaccine is a day patients like those served by Bailey are denied access to what could be the difference between life and death, between another hug with a close family member or never seeing them again.
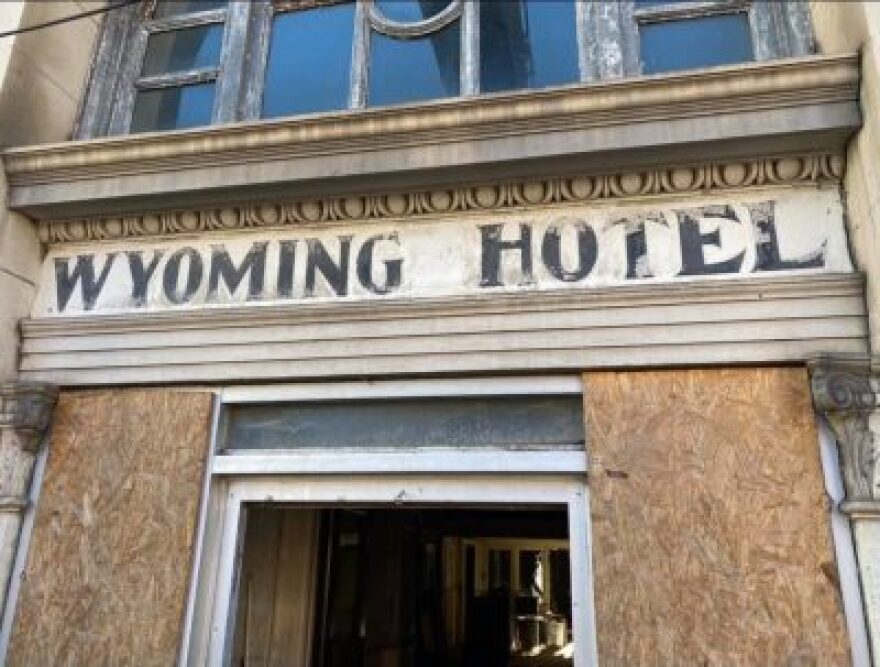
Nathan England
/
The former Wyoming Hotel in Mullens, West Virginia.
While residents of counties with clinics are afforded quick access, people like Veronica and Carl Allen from rural Wyoming County face obstacle after obstacle.
Carl, 77, used to work as a coal miner. Later, he worked doing masonry for the Department of Education.
Veronica is a former school bus driver, but after severe glaucoma left her nearly blind, she went to work at the council on aging.
“I’d look at those senior citizens, bless their heart, and I’d think one day that will be me,” Veronica said. “And here I am.”
Veronica is homebound and uses a wheelchair. She has chronic respiratory disease. Carl has suffered several strokes. He’s had a heart attack and has lung problems, and has to wear a machine to help him breathe when he sleeps.
They don’t have any family or kids, but neighbors come into their house a few times a week to help them clean and get their groceries. If either of them got COVID-19 they’d be extremely high risk.
It’s people like them who the current plan has let slip through the cracks.
If West Virginia’s latest iteration of the plan comes to fruition, there will be a clinic in Wyoming County in the next two weeks. But until that actually happens, Veronica and Carl will be waiting.
“I just hope I can get that vaccine soon,” Veronica said.
Reach reporter Lauren Peace at laurenpeace@mountainstatespotlight.org.
Add WVPB as a preferred source on Google to see more from our team
The governor’s argument centers around the Equal Protection for Religion Act, which prohibits the government from substantially burdening sincere religious exercise unless it satisfies the strictest legal scrutiny.
This week, too often, people with mental health challenges or substance use disorder wind up in jail. But crisis response teams offer another way. Also, changes to the Endangered Species Act could benefit big business. They could also kill animals like the eastern hellbender. And, in troubled times, a West Virginia writer says to find peace in nature.